
















































Low back pain is often referred to as lumbago or lumbodynia. Lumbago or "lumbago" is an attack of acute lower back pain, which is usually associated with hypothermia and exertion. Lumbago occurs in many people and is often the cause of temporary disability. Often the cause of lumbago can be sports injuries or sprains, but sometimes the factor that provokes the appearance of pain remains unknown. Lumbago is characterized by pain without radiating to the legs. Low back pain (lumbago) can appear acutely and gradually progress throughout the day. Often there is stiffness in the morning and gradually the stiffness turns into pain syndrome. Curvature of the spine (antalgic scoliosis) is also possible as a result of muscle spasm. The pain itself may be due to muscle spasm, which in turn is related to other causes. This can be overload or sprain, sports injuries, herniated discs, spondyloarthrosis (spondylosis), kidney disease (infections or kidney stones). Sometimes the patient accurately determines the causal relationship of the appearance of malaise with stress, hypothermia, but often pain appears for no apparent reason. Sometimes, back pain can appear even after sneezing, bending over, or putting on shoes. This can be facilitated by deforming diseases of the spine, such as scoliosis.
Unlike lumbago, the term lumbodynia means not acute pain, but subacute or chronic pain. As a rule, pain with lumbodynia appears gradually over several days. Pain can also occur in the morning hours and may decrease with physical activity. Lumbodynia is characterized by increased pain during prolonged static loads (sitting, uncomfortable body position). It is also characteristic of lumbodynia that the pain is relieved by lying down in a certain position. Lumbodynia patients have difficulty performing routine activities such as washing or putting on shoes due to muscle spasms. Due to the disease, there is a decrease in the volume of movements of the trunk (tilting forward or, to a lesser extent, tilting to the side or extension). Due to pain syndrome, the patient often has to change position when it is necessary to sit or stand. Unlike lumbago, muscle spasm is less pronounced and, as a rule, does not cover the entire lower back, and there are often signs of a prevalence of spasm on one side.
Causes of back pain
Back pain is a symptom. The most common causes of back pain are diseases (injuries) of muscles, bones, and intervertebral discs. Sometimesback paincan be caused by diseases of the abdominal cavity, small pelvis and chest. Such pains are called reflected pains. Diseases of the abdomen (eg, appendicitis), aortic aneurysm, kidney disease (urolithiasis, kidney infection, bladder infections), infections of the pelvic organs, ovaries - all of these diseases can manifestback pain. . . Even a normal pregnancy can lead to back pain due to sprains in the pelvic area, muscle spasm due to stress, and irritation of the nerves.
Oftenback painis associated with the following diseases:
- Compression of the nerve root, which causes symptoms of sciatica and is most often caused by a herniated disc. As a rule, when the nerve root is compressed, the pain is acute, has irradiation and impaired sensitivity in the innervation zone of the nerve root. A herniated disc occurs primarily as a result of disc degeneration. There is a bulging of the gelatinous part of the disc from the central cavity and pressure on the nerve roots. Degenerative processes in the intervertebral discs begin at the age of 30 and older. But the very presence of a hernia does not always lead to an effect on the nervous structures.
- Spondylosis - degenerative changes occur in the vertebrae themselves, bone growths (osteophytes) occur, which can affect nearby nerves, which leads to pain.
- Spinal stenosis can occur as a result of degenerative changes in the spine (spondylosis and osteochondrosis). A patient with spinal stenosis in the lumbar region may experience lower back pain radiating to both legs. Low back pain can appear as a result of standing or walking.
- Cauda equina syndrome. This is a medical emergency. Cauda equina syndrome occurs as a result of compression of the cauda equina (terminal part of the spinal cord) elements. A patient with cauda equina syndrome may experience pain and impaired bowel and bladder function (urinary incontinence and atony). This syndrome requires emergency surgery.
- Pain syndromes such as myofascial pain syndrome or fibromyalgia. Myofascial pain syndrome is characterized by pain and soreness at certain points (trigger points), a decrease in the volume of muscle movement in painful areas. The pain syndrome is reduced by relaxing the muscles located in the painful areas. With fibromyalgia, pain and soreness are common throughout the body. Fibromyalgia is not characterized by tightness and muscle pain.
- Bone infections (osteomyelitis) of the spine are rarely the cause of the disease.
- Non-infectious inflammatory diseases of the spine (ankylosing spondylitis) can cause stiffness and pain in the spine (including the lower back), which is especially worse in the morning.
- Tumors, most often cancer metastases, can be a source of lower back discomfort.
- Inflammation of the nerves and, accordingly, pain manifestations (in the chest or in the lumbar region) can be caused by damage to the nerves themselves (for example, with shingles)
- Given the variety of causes of symptoms, such as acute or subacute low back pain, it is very important to fully evaluate the patient and perform all the necessary diagnostic procedures.
Symptoms
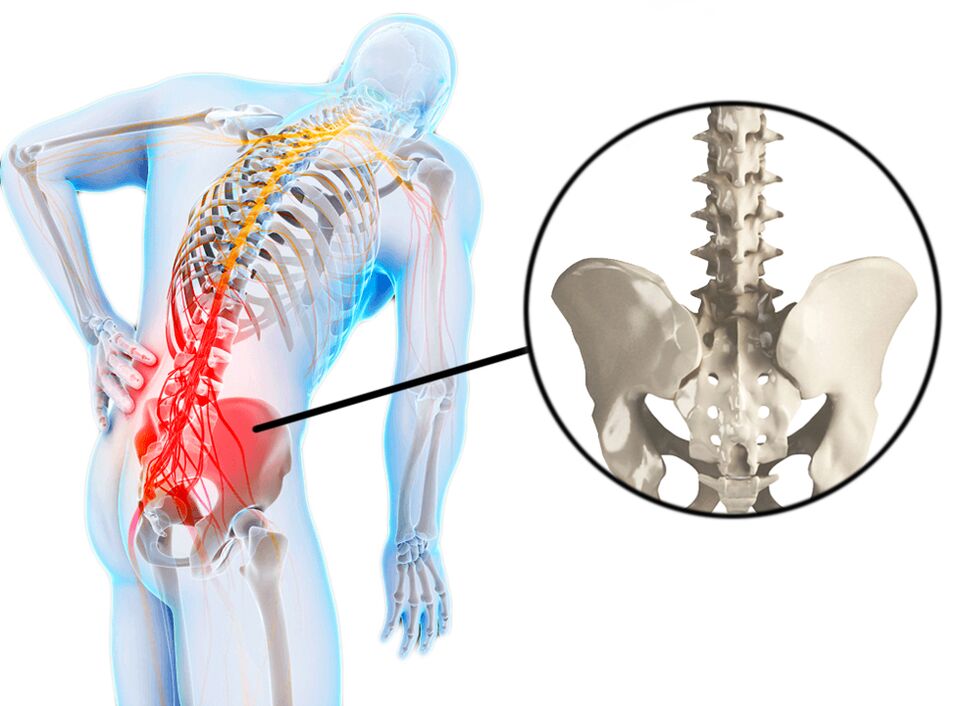
Pain in the lumbosacral region is the main symptom of lumbago, lumbodynia, lumboishalgia.
- The pain may radiate down the front, side, or back of the leg (lumboishalgia), or it may be localized only in the lumbar region (lumbago, lumbodynia).
- The feeling that the lower back hurts can intensify after exertion.
- Sometimes the pain can get worse at night or when sitting for a long time, such as during a long car trip.
- Perhaps the presence of numbness and weakness in the part of the leg, which is located in the zone of innervation of the compressed nerve.
For timely diagnosis and treatment, a number of criteria (symptoms) deserve special attention:
- Recent trauma, such as a fall from a height, a traffic accident, or similar incidents.
- The presence of minor injuries in patients over the age of 50 (for example, falling from a low height as a result of sliding and landing on the buttocks).
- History of long-term use of steroids (for example, these are patients with bronchial asthma or rheumatological diseases).
- Any patient with osteoporosis (mostly elderly women).
- Any patient over 70 years of age: at this age, there is a high risk of cancer, infections and diseases of the abdominal organs, which can cause lower back pain.
- History of oncology
- The presence of infectious diseases in the recent past
- Temperature over 100F (37. 7 C)
- Drug use: Drug use increases the risk of infectious diseases.
- Lower back pain worsens at rest: as a rule, this nature of pain is associated with oncology or infections, and such pain can also be with ankylosing spondylitis (ankylosing spondylitis).
- Significant weight loss (for no apparent reason).
- The presence of any acute dysfunction of the nerve is a signal for urgent medical attention. For example, this is a violation of walking, dysfunction of the foot, as a rule, are symptoms of acute nerve injury or compression. Under certain circumstances, such symptoms may require an emergency neurosurgical operation.
- Bowel or bladder dysfunction (both incontinence and urinary retention) can be a sign of a medical emergency.
- Failure to respond to recommended treatment or increased pain may also warrant seeking medical attention.
The presence of any of the above factors (symptoms) is a signal for seeking medical help within 24 hours.
Diagnostics
Medical history is important for making an accurate diagnosis, as various conditions can cause lower back pain. The timing of the onset of pain, the relationship with physical exertion, the presence of other symptoms such as cough, rise in temperature, dysfunction of the bladder or intestines, the presence of seizures, etc. A physical examination is carried out: identification of pain points, the presence of muscle spasm, a study of the neurological status is carried out. If there is a suspicion of diseases of the abdominal organs or pelvic organs, then an examination is carried out (ultrasound of the abdominal organs, ultrasound of the pelvic and pelvic organs, urine blood tests).
If the somatic genesis of lower back pain is excluded, then instrumental research methods such as radiography, CT or MRI can be prescribed.
X-ray is the initial examination method and allows you to determine the presence of changes in bone tissue and indirect signs of changes in the intervertebral discs.
CT allows you to visualize the presence of various changes, both in bone tissue and in soft stones (especially with contrast).
MRI is the most informative research method that allows diagnosing morphological changes in various tissues.
Densitometry is necessary when osteoporosis is suspected (usually in women over 50)
EMG (ENMG) is used to determine the violation of conduction along nerve fibers.
Laboratory tests are prescribed (blood tests, urine tests, blood biochemistry) mainly to exclude inflammatory processes in the body.
Pain treatment

After the diagnosis and confirmation of vertebral genesis with lumbago and lumbodynia is established, a certain treatment for lower back pain is prescribed.
In acute pain, rest is necessary for 1–2 days. Bed rest can reduce muscle strain and muscle spasm. In most cases, when the pain syndrome is due to muscle spasm, the pain syndrome decreases within a few days without the use of drugs, only due to rest.
Medication. For pain syndrome, drugs of the NSAID group are used. COX-2 inhibitors have fewer side effects, but long-term use of these drugs also has certain risks. Given that all drugs in this group have a lot of side effects, taking drugs in this group should be short-lived and under the mandatory supervision of a physician.
Muscle relaxants can be used to relieve spasm. But the use of these drugs is effective only in the presence of a spasm.
Steroids can be used to treat pain, especially when there are signs of sciatica. But due to the presence of pronounced side effects, the use of steroids should be selective and short-lived.
Manual therapy. This technique can be very effective in the presence of muscle blocks or subluxation of the facet joints. Mobilizing the motor segments can reduce both muscle spasm and lower back pain.
Physiotherapy. There are many modern physiotherapy procedures that can both reduce pain and inflammation, improve microcirculation (for example, electrophoresis, cryotherapy, laser therapy, etc. ).
Exercise therapy. Exercise is not recommended for acute lower back pain. The connection of exercise therapy is possible after reducing the pain syndrome. In the presence of chronic pain, exercise can be very effective in strengthening the muscle corset and improving the biomechanics of the spine. Exercises should be selected only with an exercise therapy doctor, since often independent exercises can lead to increased pain manifestations. Systematic exercise therapy, especially in the presence of degenerative changes in the spine (osteochondrosis, spondylosis), can preserve the functionality of the spine and significantly reduce the risk of pain syndromes.